What is the Tailbone?
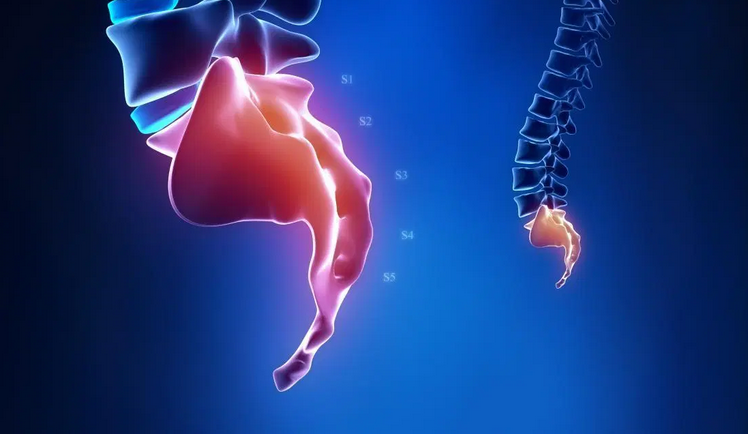
The coccyx, or tailbone, is the last piece of the spine. It’s shaped like a triangle, and attaches to the sacrum by ligaments that run front, back, and both sides. To find your tailbone, just feel down your back, between the buttocks, until just above the opening of the anus.
In a healthy alignment it is mobile (moves slightly when pressed upon), center line, pain free, and continuous with the sacrum. However in a dysfunctional alignment it may be painful to touch it or the tissue around it, immobile, and even noticeably off-center. It may feel like it “points” deep into the body, rather than continuous with the rest of the spine.
See more here Also here and here



Function of the Coccyx
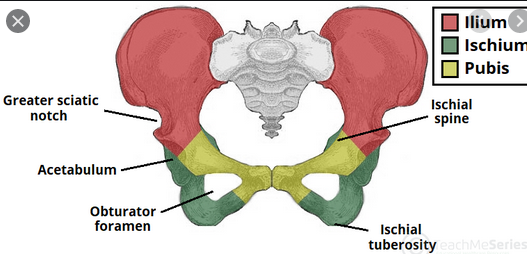
Although the tailbone is considered vestigial (or no longer necessary) in the human body, it does have some function in the pelvis. For instance, the coccyx is one part of a three-part support for a person in the seated position. Weight is distributed between the bottom portions of the two hip bones (or ischium) and the tailbone, providing balance and stability when a person is seated. The tailbone is the connecting point for many pelvic floor muscles. These muscles help support the anus and aid in defecation, support the vagina in females, and assist in walking, running, and moving the legs.
Joints
The coccyx articulates with the sacrum at a fibrocartilaginous joint called the sacrococcygeal symphysis.
Movement here is limited to minor flexion and extension which occurs passively, for example during defecation and labour.
Ligaments
The sacrococcygeal symphysis is supported by five ligaments:
- Anterior sacrococcygeal ligament – a continuation of the anterior longitudinal ligament of the spine, and so connects the anterior aspects of the vertebral bodies.
- Deep posterior sacrococcygeal ligament – connects the posterior side of the 5th sacral body to the dorsal surface of the coccyx.
- Superficial posterior sacrococcygeal ligament – attaches the median sacral crest to the dorsal surface of the coccyx.
- Lateral sacrococcygeal ligaments – run from the lateral aspect of the sacrum to the transverse processes of Co1.
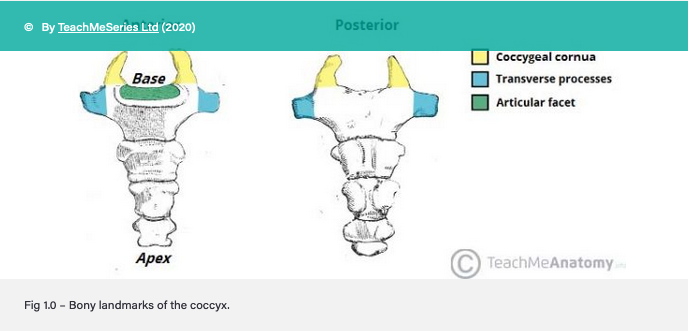
- Interarticular ligaments – stretch from the cornua of the sacrum to the cornua of the coccyx.
Attachments
One of the key functions of the coccyx is as an attachment point for various structures. The gluteus maximus attaches to the coccyx, as does the levator ani muscle, which is a key component of the pelvic floor. The anococcygeal raphe is a thin, fibrous ligament which runs from the coccyx and helps support the position of the anus.
SELF HELP – the ‘lifters’
What it all is and does – deep pelvic floor muscles . .
- 10 minutes in – how to help – and to assist she says – to get ready for birthing
- Remember that she is not ‘setting it up to win’ . . .
- 15.45 – women tend to hold in stomach . . soft belly/’think like dogs’
- 16.45 – painful sex – esp from behind . . jamming into the tight muscles – not happy!
- 18 – Why the whole body gets upset when we have ONE area is distressed.
Another version
Do NOT need a PT physical therapist – they need to find YOU – as the womb is not happy and why not???
Gentling Way . . .
- 2.30 – actual exercise . . (Why not fix it??)
- If you have broken tailbone- will hurt even more trying to get up from seated – than it was sitting down – and lasts – in my case – for over 10 years – till GV 1 was inserted.
Another men’s version – there is a cadaver pic – be warned. .
Misalignment causes – just about everything.
Chronic lower back discomfort. Stiff neck. Pelvic floor dysfunction such as pain with intercourse or urinary incontinence. Inability to sit squarely or for long periods of time. Pain with bowel movements. What’s the connection? The tailbone. Also vulvadynia and all pelvic related pain will have an aspect – at least secondarily if not the primary cause – and then there is . . inflammation
How to avoid? (inflammation)
Drink more water – always – more Vit D3 and magnesium – 20 x daily at least till no more pain – and sleeping digestion, tension and all emotional issues will also lessen.Avoid ALL sugar and anything that converts to this includes all grains and potato and fruits not only chocolate and sweets. . (And dairy and alcohol).
What is worse – being in constant pain – fighting off all ‘fixers’ – but not actually undoing it.
How did it happen?
Although it is a common site of injury, often taking the brunt of our many childhood and adult slip and falls, the tailbone is unfortunately an under-evaluated source of pain and dysfunction in both men and women. Once injured it can cause pain in sitting, pain with bowel movements, pelvic floor dysfunction, (such as pain with intercourse) or even cause reactions up the spine, all the way to the neck and head.
What the Problems Associated with Tailbone Misalignment?
The most obvious symptom is coccydynia, or pain at the tailbone. However often patients have no pain at the tailbone until it is directly touched, and occasionally have no pain around it at all. This symptom may manifest as an inability to be comfortable in sitting. Often patients find themselves shifting from buttock to buttock in search of a comfortable position.
Pelvic floor dysfunction is common, as the pelvic floor muscles attach around the tailbone. Their ability to function optimally is affected by the positioning of the bones around them. Problems may include pain with intercourse, sensation of “tightness,” or pain with bowel movements. Bladder leaking may be aggravated by the inability of the pelvic floor to contract optimally.
Pain or tightness further up the spine is often a secondary symptom that patients don’t realize is connected. Since the spine and its contents are continuous from the skull to the tailbone, a tailbone out of place can affect alignment all the way up to the head. The most common two places I see this are the lower back and the suboccipital region, or area just below the skull on the back of the neck. Chronic nagging pain or tightness in these areas that shifts but never resolves despite care may be traced down to malalignment of the tailbone.
Structure Determines Function
Having had a broken tailbone at 12 years old and again about 16 years ago, I know what to ask for.
(To decide whether badly broken, or ‘just’ bruised – maybe dislocated forever . .
Did it hurt more to get up than to sit down (both excruciating initially).
If yes – is /was broken – and often stays problematic in seating and getting up again – forever after – until we rescue.
Eg – Mrs Chen and 30+ years story.
Also my own – thus I knew what to do.
Then there is what travels though the Alcock’s canal – pudendal nerve.
A case – from the class (CLICK)
MOVES – anything that undoes the Stuck Liver Qi
All moxa and any sacral and glut moves will loosen off what is holding the tension/distress.
Perineal steaming and acupoint GV 1– all needs setting up.
All sacral moves will assist greatly – and repeat them all further down . .
Specific
Coccygeal stretch – Numerous ways.
- 1 – Locate tip of the coccyx
- 2 – Place thumbs next to this and use gentle upwards pressure.
Hortence’s point (“a miniscule area on the ischial ramus…that brings great relief to many female complaints when palpated according to her instructions”) – From Miss Hortence in Belize
- 1 – Locate the top of the coccyx. This in itself may be a mission – sometimes it is broken and reset off to a side, deeply underneath where it would normally be, or in one I discovered (Josi) set back by at least a cm – depressed towards the pelvis. An old ice shaking injury – resulting in 4 breeches.
- 2 – Laterally move 2-3 fingerbreaths against the gluteal muscle.
- 3 – Gently slide the fingers into the ‘half non’ bone.
- 4 – Apply gentle pressure in three areas on the bone – each end and at the middle.
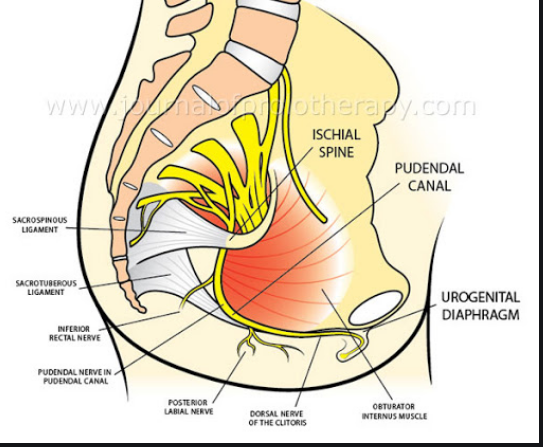
Hortence’s point – we affect the sacrotuberous ligament (integral to pelvic stability). Scroll down on this site to see a video of a pelvis model placed over and actual live body as Til Luchau (longtime rolfing teacher) demos and describes how to palpate this area. See more here
The pudendal nerve that flows through Alcocks Canal aka Hortences – innervates the cervix and the clitoris.
Nerve roots are– S2-S4. Sensory – innervates the external genitalia of both sexes and the skin around the anus, anal canal and perineum. Motor – innervates various pelvic muscles, the external urethral sphincter and the external anal sphincter.
Damage to the sarcrum and sacral nerve can effect the pudendal nerve as well. USE THIS point with any lower back injuries or in those who sit a lot. It gives great relief, and connects folk with feelings of release and pleasure post treatment.
See here (CLICK) – About 8 minutes in he is talking about how to help #coccyx. .
WARNING pilonidal cyst . .
A pilonidal (pie-low-NIE-dul) cyst is an abnormal pocket in the skin that usually contains hair and skin debris. A pilonidal cyst is almost always located near the tailbone at the top of the cleft of the buttocks. Pilonidal cysts usually occur when hair punctures the skin and then becomes embedded. (‘Nest of hair’) – may get infected to become an abscess.
Remember – where is the iodine – if it is a cyst???
- 2.20 – tiny ‘water’ filled balloon.
Think Silica . .all forms .. and what allows this into the cell membrane (that we in health do not have)?
red clover tea – 2 cups daily – simmered not steeped.
Castor oil packs
Steaming may assist with x2 daily self care self soothing and lymph drainage and all else we have done in the earlier classes.
Soaking in warmth – castor oil and STEAMING!!
And WHY IS IT THERE – that is the question . . .
Risk factors for pilonidal cysts include the following:
(Most experts believe that the cysts arise due to trauma to the area that results in ingrown hairs. Pilonidal cysts often contain hair when excised, but hair follicles have not been demonstrated in them, suggesting that the hair may have been introduced from outside the cyst. Pilonidal disease was a common problem among servicemen during World War II, thought to be due to the mechanical trauma of riding in jeeps, trucks, and tanks.)
- Male predominance (four times more often than in women)
- Young age (most commonly found in men in their 20s)
- Sedentary lifestyle
- Thick body hair
- Family history
- Local shaving or damage to the skin from friction
- Overweight or obese
- Previous pilonidal cyst
- The story from a young sufferer
(” not a cure – only doctors can CURE things’ – says he. . )
Not the body healing itself . . (the 5th ‘L’)
Making a white vinegar and baking soda paste. (This only happens in that location here . ).
My thoughts – he needs to fix up why it is there – damp and heat if a TCM inclined person
The scar and adhesions will need sorting out . .
Please note – who is speaking of gyno visceral work?
That is the start of it all – back to the Liver and ligaments and emotions . .

Bowen coccyx correction
Bowen coccyx correction – part 2
Opening the baby gate – to get ready to let go baby
Steaming first – at least moxa sacral fan – make it easier for everyone involved
Se