Welcome

Maybe see here first? – Videos of me explaining the process of healing after this has happened.
and now we move onto what I found when looking for the historical perspective – what happens later on in a woman’s body after C section?
What might have been – replaced by at the very least – inadequate flows.
Possibly massive body disruption and a life of unresolved STUCK (that ‘T’ word).
Specifically – though the other abdominal incursions can also lead to these – though may be not as obvious – as the layering up after Bonsai’ing a woman’s body takes some undoing.
And of course, she has responses to all of this. .
Here is what I found – after effects – seem only to be ‘on their’ watch – the surgeons and till she gets home
Cesarean section one hundred years 1920–2020: the Good, the Bad and the Ugly – good read
1970–2020 – In the 1970s, an upsurge in the CS rate was observed, justified on the basis of maternal and fetal results and safety improvement. The rate, from 5.5% of deliveries in 1970 to 16.5% in 1980, continued to increase until appearing to have stabilized around 31–32% in the US in 2019
STATS AND FACTS – https://www.statista.com/topics/5217/cesarean-sections/
Who will be birthing as their projected 2030 rates are eclipsed by reality in UK, USA, Aust and NZ – and no doubt most other ‘affluent’ countries – CAN WE AFFORD THIS? more babies were born through surgery than vaginally. C-sections can be planned, but are often unplanned when unexpected problems arise during a vaginal delivery which could put the mother or baby at risk. A C -section can be life-saving and is medically necessary in situations such as having a ‘low-lying’ placenta, a ‘breech’ baby, prolonged or obstructed labor, or when there is fetal distress. However, it is still a major surgery and involves both short-term and long-terms health risks for the mothers and babies. For example, the potential for heavy bleeding or infection, slower recovery times after childbirth, delays in establishing breastfeeding and skin-to-skin contact, and increased likelihood of complications in future pregnancies. Therefore, the WHO recommends the reduction of medically unnecessary cesarean sections such with as low-risk first time mothers. Yet, the rate of cesarean deliveries is increasing in every region around the world. Global rates are projected to reach 28.5 percent by 2030.

VERY DISTURBING – and not informed at the opportunity to do so – the C section seems easy . . BUT what about the EFFECT ON CHILD (2020)
Conclusions “This systematic review of literature and meta-analysis shows, that cesarean section may be associated with several pediatric complications. The results of the studies included indicated that children delivered by cesarean section more commonly developed respiratory tract infections, obesity and the manifestations of asthma than children delivered vaginally. The risk of developing diabetes mellitus type 1 or neurological disorders in offspring after caesarean section is still under discussion. Due to a high number of reciprocally exclusive study results concerning long–term pediatric sequelae it is recommended to conduct a multic-enter prospective study comprising the concept of epigenetic influence of cesarean section”.
See here for a ‘case’ of twins – one birthed, one cut out – bearing in mind that he was under duress as the mum was in trouble – so was with Ryan – both had ‘issues’ leading into saving his life – and his mum’s.
The seeding is needed because – ‘The disturbed colonization with bacterial microflora within the skin and digestive tract was the reason for a more frequent occurrence of immune diseases in children delivered by cesarean section’.

REMINDER – HOWEVER – I would not be here without this being done – so to be taken in context – the baby also would not be.
HE was put in the humidicrib, and was unable to maintain body temp till the OLDER MIDWIFE (voice of reason) said, put him next to mum.
BUT also – he was almost killed by their ineptitude with thumping me on the diaphragm, hard – not once but twice – which of course ruptured the clot, and he was also transverse – and it would have been all systems – HELP – and he did not get his cord blood, he was issued with not only the usual anesthetic but before this – two lots of adrenaline as my B.P. got lost, and without ME knowing what to do – ME – and the fact of both my friends/helpers in theatre were past acup students of mine, and we have needles with us – Jane inserted left St 36 and my B.P. was instantly back – all need to know, and carry pricklies to save yourself – that was only ONE time I did.
From here – ‘Time to consider the risks of caesarean delivery for long term child health’
NOTE – Maternal request for C section is NOT being baby friendly/respectful. Rates of caesarean section are rising, with maternal request and repeat caesarean accounting for a large proportion in some countries Caesarean delivery has been linked to increased risk of childhood obesity, asthma, and type 1 diabetes The evidence on these risks has not been reviewed in clinical guidelines. Knowing about child health risks could change decisions when caesarean is not a medical necessity
This page is about mum – so that is all I am adding on here – you can go looking yourself:
mostly on chiro sites as they deal with the neurological which are substantial.
I searched for ‘C section complications’ on Google mid August 2025 – and hardly any mention of how to live with your body forever after the CS . .
A good place to get an overall idea – complications – mum and baby
https://americanpregnancy.org/healthy-pregnancy/labor-and-birth/c-section-complications/?nocache=1706571081
General info offered – ‘If a C-section is planned, your healthcare team will provide specific instructions to prepare for the procedure. This may include pre-surgical evaluations, fasting, and medication changes. The surgery includes:
- Anesthesia—typically a spinal block or epidural
- Incision—a horizontal incision is made across the lower abdomen. The uterus is then opened to deliver the baby.
- Delivery—after the baby is delivered, the umbilical cord is cut, and the placenta is removed.
- Closure—the uterus and abdomen are sutured.
How Long Does a C-Section Take? The entire procedure typically lasts 45 to 60 minutes.
What Is Recovery from a C-Section Like?
Recovery from a C-section usually takes longer than recovery from vaginal birth. Here’s what to expect:
- Hospital stay: Most parents stay for 2 to 3 days.
- Pain management: Medications may be prescribed for incision pain.
- Activity restrictions: Avoid lifting heavy objects or strenuous activity for 6 weeks.
- Follow-up: A post-operative check-up is usually scheduled 2 to 6 weeks after delivery”.
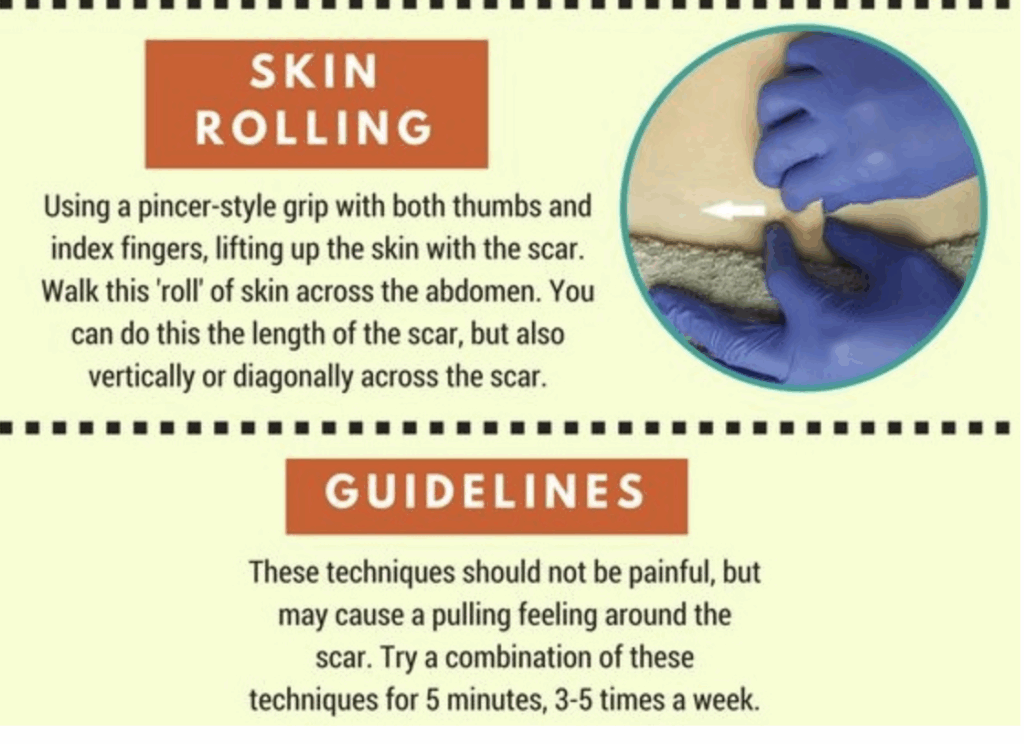
I found this on a site somewhere – refer to my Unblocking Your Scar workshop – see more here

From one article.- ‘Acute haemorrhagic complications include retained products of conception, subfascial and bladder flap haematomas and, rarely, postpartum uterine dehiscence or rupture and iatrogenic vascular complications. Infective complications include puerperal and wound infections’.
Me – All seem only interested in pregnancy and childbirth after C section but we also have to LIVE in that body from then on.
Common sense – Conclusion: Pre- and post-operative complications of cesarean section delivery during labour (i.e., emergency cesarean) increase with the degree of labour emergency. It would be ideal to identify women in labour who are at increased risk of emergency cesarean earlier, so that the situation does not escalate to a red code cesarean.
From here – “The increase in cesarean section (CS) rates, whether they are classified as unnecessary or elective, has globally raised significant concerns due to the associated risks involving maternal and neonatal outcomes. Although CS can be a lifesaving operation in specific medical cases, its overuse is exposing mothers and neonates to complications like hemorrhage, infections, and long-term consequences such as uterine scarring, infertility, and future pregnancy problems”.
WORTHWHILE ARTICLE TO READ https://pmc.ncbi.nlm.nih.gov/articles/PMC9807024/
Even with ‘bright’ women – they have not much awareness of C section complications and would prefer a normal birth
MAY I ADD – who seems to care about the woman’s life after C section when reproductive history is over?
Esp adeno myosis and the need for hysterectomy after the surgical incursion that was not that needed?
One of the best sites I found (15 pages into google) – first time I found mention of adhesions also DOES NOT mention – as none of them do – life after.
List given of immediate after effects of C section Pain, bleeding, infection, blood clot, adhesions, affects on future fertility, ONLY
WHAT ONE PAGE SAYS – pregnancy after C section . . ..
All of these need the Easy Pregnancy Solutions (with $50 more for ALL the eBooks) and the scar workshop = to gently undo themselves at any stage
WHAT WE DO NOT NEED
USEFUL TO READ – https://www.sciencedirect.com/science/article/abs/pii/S0140673618319305
Key messages • 1) – Infants born by CS have different hormonal, physical, bacterial, and medical exposures (such as intrapartum antibiotics and uterotonins) and are exposed to more short-term risks, which range from altered immune development, allergy, atopy, asthma, and reduced diversity of the intestinal gut microbiome, compared with those born vaginally.
2) •Caesarean section (CS) is a life-saving intervention for specific complications during pregnancy and childbirth that should be available to all women in need. CS also confers an increased risk of maternal mortality and severe acute morbidity and a higher risk for adverse outcomes in subsequent pregnancy compared with vaginal birth. Multiple CSs are associated with a higher risk of maternal morbidity and mortality.
3) •Some benefits of CS, such as less frequent incontinence and urogenital prolapse have been described.
4) – Conclusions “Almost every woman who has a CS increases her risk of certain morbidities in her subsequent pregnancies. The axiom once a caesarean, always a caesarean is not evidence-based, but once a caesarean, always a scar reinforces the maxim that women with a previous CS should be considered to be at increased risk of obstetric complications and poorer outcomes for mother and baby. The discussed evidence shows the complexity in achieving an initially favourable result from an operative intervention.
GREAT ARTICLE ALSO – Abstract: Background: Vaginal birth and cesarean section (CS) are the primary delivery modes, each with distinct short- and long-term maternal health outcomes. Understanding these differences aids in informed delivery planning. Objective To evaluate and compare the short- and long-term maternal health outcomes of vaginal births versus cesarean sections among patients at Barasat Government Medical College. Methods: A prospective cohort study was conducted on 100 patients (vaginal birth: n=60; CS: n=40) between January 2023 and December 2024.
Results: Recovery within five days was achieved by 75% of vaginal birth patients compared to 30% of CS patients (p<0.01). Infection rates were 10% in vaginal births and 25% in CS cases, including surgical site infections (20% in CS). Severe postpartum pain was reported in 15% of vaginal births versus 40% of CS patients. Perineal trauma occurred in 18% of vaginal births, while 5% of CS cases had abdominal wound dehiscence.Long-term, pelvic floor disorders were higher in vaginal births (12%) compared to CS (5%). Subsequent pregnancy complications occurred in 32% of CS patients, including uterine rupture (12%) and placenta accreta (15%), compared to 5% in vaginal births. Chronic pelvic pain was reported in 20% of CS patients versus 8% in vaginal births Conclusion: Vaginal birth promotes faster recovery and fewer surgical risks, while CS poses significant long-term reproductive risks. Individualized care decisions are essential for optimizing maternal health.
ADVICE ON PREGNANCIES AFTER – and waiting – not one is talking about nutrition or mention undoing the reasons ‘needed’ for the initial C section.
‘CARE’ after C section – https://www.verywellhealth.com/c-section-scar-healing-stages-8383850 see all on my work preferably
On the 16th google page I find https://www.antenatals.com/blog/what-are-the-most-common-c-section-recovery-problems/
Recovering from a C-section can be challenging, both physically and emotionally. The most common recovery problems include incision pain, swelling, difficulty with bowel movements, uterine discomfort, and emotional challenges like postpartum depression or trauma.
Still – is only after operation – not down the track.
https://unmhealth.org/stories/2022/10/c-section-recovery-whats-normal-when-to-call-doctor.html
https://www.mayoclinic.org/tests-procedures/c-section/expert-answers/c-sections/faq-20058380
The more C-sections, the higher the risk of problems with the placenta, including:
- The placenta implanting too deeply into the uterine wall. This condition is called placenta accreta.(DEADLY)
- The placenta partly or completely covering the opening of the cervix. This condition is called placenta previa.(DEADLY)

Serious bleeding.
The need for blood transfusions.
The need for surgery to remove the uterus, called hysterectomy.
Health issues related to surgery, such as organ and tissue damage.
The need for an emergency delivery.
These conditions raise the risk of: Preterm delivery.
How many C sections to be OK? Depends entirely on your nutrition and care of the scar/body – as the GV woman who had over 10 in 13 years – and what a test of life!! She is only here still due to her diligent doing all I said to. HER BELLY ON THE RIGHT – after my adhesion breaking.
She felt vastly lighter – as you do . .ungluing self.
In Saudi Arabia – 5-9 CS against less than https://pubmed.ncbi.nlm.nih.gov/15383111/ Conclusion: The higher order (5-9) repeat caesarean sections carry no specific additional risk for the mother or the baby when compared with the lower order (3 or 4) repeat caesarean sections.
NO ONE SAYS BOO ABOUT THE LONG TERM BODY WOUNDING OF THIS
https://parenting.firstcry.com/articles/multiple-or-repeat-c-sections-benefits-and-risks/
WHAT ABOUT THE MORBIDLY OBESE PREGNANT WOMAN? (over 40 BMI) https://pmc.ncbi.nlm.nih.gov/articles/PMC3289484/
IMPORTANT – see what this site has on it.
Page 20 of Google – clear passage – a version of what we do . .
ADHESIONS AND WHY WE ARE WORKING AS WE DO
Adhesion prevention after cesarean delivery: evidence, and lack of it
In spite of the recognized occurrence of cesarean-attributable adhesions, its clinical significance is uncertain. The presence of adhesions during a repeat cesarean section can make fetal extraction lengthy and the procedure challenging and may increase the risk of injury to adjacent organs. Two methods for adhesion prevention are discussed, peritoneal closure and use of adhesion barriers. Peritoneal closure appears to be safe in the short term. In the long term, conflicting evidence arise from reviewing the literature for possible adhesion reduction benefits. A systematic review of the literature on the use of adhesion barriers in the context of cesarean section yielded only a few studies, most of which are lacking in methodology. For now, it appears that the available evidence does not support the routine use of adhesion barriers during cesarean delivery.
HERE WE HAVE – To compare the obstetric outcomes of cesarean section in women who had a history of four or more previous cesarean sections with those who had a history of two or three previous cesarean sections. In conclusion, repeated CSs (four or more) do not appear to increase the risk of maternal complications except for the rate of intra-abdominal adhesions. Although there is no remarkable difference in serious morbidity associated with MRSC, it should be kept in mind that CS is a operative delivery including some risks such as uterine rupture, infection, hemorrhage, thrombosis and peripheral organ damage. Further studies are needed to make a recommendation to women on the maximum number of CSs which should be performed.
WHAT TO EXPECT IN HEALING – RECOVERY TIPS no mention of after the immediate time – again – the older woman and her continuing sagas.
What od o? Steaming, belly binding, AND faja, castor oil up inside, on sacrum and on belly and in vagina – and nutrition to improve not only milk, and life, but sort out the missing ingredients that are keeping baby and mum ‘OK’ not healing her long term . .
Supposedly – https://www.intechopen.com/chapters/89254 VERY USEFUYL TO ERAD _) is on page 17 of Google – and is the best so far
Maternal issues – Increased risk of placenta previa, placenta accreta, and placental abruption in subsequent pregnancies, Increased risk of miscarriage, Uterine rupture risk Pelvic floor dysfunction, Chronic pain and adhesions, Stillbirth in subsequent pregnancy, Possible association with certain cancers, such as cervical cancer. DOES NOT MENTION NEED FOR EMERGENCY HYSTERECTOMY as they can’t stop heamorrhaging.
Conclusion – (ME – as usual – who cares about mum after she leaves the postnatal time?)
Despite their lifesaving role, unnecessary cesarean sections expose mothers and babies to avoidable risks. Although various factors can lead to a cesarean, vaginal birth remains possible in many cases. The decision ultimately depends on factors such as maternal health, fetal well-being, and available resources. The steady increase in cesarean section rates, particularly elective cesareans, warrants attention. Further research should be conducted to inform policymakers and program planners on strategies to control unnecessary costs and potential long-term impacts on quality of life.
LONG TERM SCAR ISSUES
Side effects of C section years later
Complications and Side effects of C-sections vary from woman to woman. It depends on the type of procedure, and on the patient’s health conditions. Following are the common problems and Long term complications after C-Section.
- Pain in the abdomen or at the incision site
- Restriction and pulling sensation around the scar and incision line
- Intermenstrual bleeding
- Chronic pelvic pain
- Risk of secondary infertility and future pregnancies
- Uterine rupture during later pregnancy (risk of incision scar tearing)
- Placenta Previa (Placenta low in the uterus)
- Hypertrophic scar and keloid formation (A thick, raised, and irregular scar at the incision line)
- Prolonged numbness around and at the incision site due to Nerve damage
Finally found on page 22 of Google. https://www.frontiersin.org/journals/surgery/articles/10.3389/fsurg.2024.1381449/full
Things you did not think of that MAY happen. Management and prevention of long-term complications related to the niche in the uterine cesarean section scar. Cesarean section [CS] is the most common major surgical procedure performed worldwide. According to WHO currently 20% of deliveries are by cesarean section, while in the European Union this percentage has already reached 30% (1).
Like any surgery, CS has its bright and dark sides. The positive aspect of CS is that it allows safe delivery in the event of maternal and/or fetal complications and contraindications to vaginal delivery. Cesarean section should be seen as an intervention that saves life and health of mother and fetus. However on the other hand CS is associated with short- and long-term complications. Short-term complications, as with any abdominal surgery, include postoperative pain, complications of anesthesia, surgical wound infection, thromboembolism, haemorrhage and many others. Long-term complications are much more specific to CS. They include complications related to the uterine CS scar, and abdominal CS scar. Uterine scar complications after CS are related to incomplete healing of the uterine wall at the incision site. This incomplete healing leads to formation of a niche. A niche is defined by the European Niche Taskforce as an indentation at the site of a Cesarean section scar that is at least 2 mm deep (2). The presence of an incompletely healed uterine CS scar (i.e., a scar with a niche) can cause complications both in subsequent pregnancies and in non-pregnant women.

In pregnant women, these complications may be life-threatening and include cesarean scar pregnancy, cesarean scar dehiscence or rupture and placenta previa accreta (3, 4). In non-pregnant women the presence of a niche leads to a group of symptoms recently named Cesarean Scar Disorder (CSDi) (5). CSDi includes such symptoms as: postmenstrual spotting, pain during uterine bleeding, technical issues with catheter insertion during embryo transfer and unexplained subfertility. Given the increasing number of CS, and thus the growing population of women with incompletely healed CS scars, measures should be taken to adequately diagnose and treat the uterine niche.
C SECTION DEFECT – SEE MORE HERE ) in 20-80% of those having more than ONE CS!! IS now called ‘niche; for short!!!
How common is CSD ? The prevalence of CSD is not known, but may be more common than realised. It has been reported amongst 20 to 80% women after 1 or more previous C-Section. What are the potential clinical implications of CSD? The majority of women who are found to have a CSD defect on ultrasound do not encounter or report any problem. However, in a small percentage of women with CSD, they may encounter a variety of clinical problems Although the causal relationship between C-Section defects and related symptoms has not been established, treatment has been reported to be successful in the resolution of symptoms.
- CSD-related abnormal implantation: ectopic pregnancy in the CSD (SCAR), placenta previa, accreta, percreta, scar rupture.
- Abnormal uterine bleeding: post-menstrual spotting
- Pain: pelvic pain, period pain, painful sex
- Secondary infertility and failed IVF: blood inside the CSD could affect the cervical mucus and sperm quality, obstruct sperm transport and impair embryo implantation
A rare but serious complication associated with uterine CS scar is a cervicovesical fistula. The fistula is most often the result of an intraoperatively unrecognized bladder injury. The most common risk factor are adhesions from previous CS procedures. Symptoms can vary depending on the location and size of the fistula and mainly include hematuria during menstrual bleeding and transvaginal urine leakage
A serious complication in this group is scar endometriosis, also referred to as abdominal wall endometriosis (AWE). AWE results from direct implantation of endometrial tissue into abdominal wall structures at the time of CS. The AWE develops in only 0.03%–1% of women after CS. However, given that 30 million CS are performed annually worldwide, the population of women with AWE is growing rapidly. Symptoms mainly include a palpable tumor and cyclic pain. Most AWE is localized in the subcutaneous fat tissue above the fascia, but there is a growing number of patients with extensive disease in which AWE involves the fascia, abdominal muscles, peritoneum and even bladder wall.
Another complication associated with abdominal CS scar is the very rare possibility of IUD migration from the perforated uterine cavity into the abdominal wall structures.
Some truth finally – https://www.researchgate.net/publication/374556566_COMPLICATIONS_AND_RISKS_OF_CESAREAN_BIRTH
Conclusions: Cesarean section is the cause of up to three times higher maternal mortality rate compared to vaginal birth, either directly or by contributing to the existing risks. Common early maternal complications are postpartum hemorrhage, wound infection, and prolonged hospital stay. After a previous cesarean birth, a trial birth should be performed in institutions with 24-hour surgical services and under the constant supervision of qualified experts. Cesarean delivery in twin pregnancies is associated with increased maternal and fetal morbidity and mortality.
SEVERE SMALL INTESTINAL OBSTRUCTION – https://pmc.ncbi.nlm.nih.gov/articles/PMC7876740/ (years later) – Caesarean section is the most common abdominal surgery performed on women worldwide. Adhesions represent a severe complication of cesarean section and can cause different degrees of bowel obstruction.
Cesarean scar pregnancy (CSP) is an abnormal implantation of the gestational sac in the area of the prior caesarean delivery (CD) scar, potentially leading to life-threatening complications, including severe haemorrhage, uterine rupture and development of placenta accreta spectrum (PAS) disorders.
Not what you want. A general conversation on this potentially fatal situation See more here – mainly for specialists – but – you may want to know.
Searching for long term problems for woman after C section – page 3 Long-term effects of cesarean sections:
ectopic pregnancies and placental problems https://pubmed.ncbi.nlm.nih.gov/9065131/
Incisional hernia – Not mentioned anywhere – any surgery and floppy QI and flesh add in cold – connective tissue – could result in – https://www.verywellhealth.com/what-is-incisional-hernia-3157228
BACK TO C SECTIONS – From https://wellwisp.com/what-are-long-term-side-effects-of-cesarean-section/
An abstract – The rapid rise in the number of caesarean deliveries has led to new iatrogenic long-term obstetric and gynaecologic complications, which are reviewed in this chapter. The main obstetric complications in pregnancies following a caesarean section include increased risks of unexplained stillbirth, placenta praevia, placenta accreta, and abruptio placentae. The risk of placenta praevia increases as the number of prior caesarean deliveries increases. The failure of the placenta to separate normally from the uterus during delivery in placenta accreta is associated with major post-partum haemorrhage; therefore, antenatal diagnosis of this condition is pivotal to ensure that delivery can be planned to occur in a tertiary care centre. Long-term gynaecological complications include a scar defect which can be associated with postmenstrual spotting, dysmenorrhoea, caesarean scar ectopic pregnancies, and pelvic adhesions which are associated with chronic pelvic pain and a decreased fertility rate.
From here – https://jccpractice.com/article/comparing-vaginal-birth-vs-cesarean-section-short-and-long-term-maternal-health-outcomes-188/
Pelvic floor, chronic pelvic pain, Subsequent Pregnancy Complications. Long-term outcomes revealed higher rates of pelvic floor disorders in vaginal birth patients (15%) compared to cesarean section patients (5%). However, cesarean section patients experienced more complications in subsequent pregnancies (30%) than vaginal birth patients (5%), including uterine rupture and placenta accreta. Chronic pelvic pain was more common among cesarean section patients but not significantly different.
From here – https://www.degruyterbrill.com/document/doi/10.1515/jpm-2020-0305/html
CONCLUSIONS – For the past hundred years there has been a continuing evolution of the role of cesarean births in obstetrics. CSs remain the most common operation performed in women of childbearing age in the world, accounting for one in three American women, and is the leading cause of maternal mortality and morbidity in the US. The operation can be life-saving for the fetus, the mother, or both in rare cases. Before the recommendation of a CS and prior to its performance however, the justification including potential risks and benefits should be provided to the patient and discussed. Potential injuries should refer to both maternal and fetal risks. The most catastrophic maternal risks are uterine rupture, excessive blood loss that may result in hysterectomy or transfusion, injury to neighboring organs (bladder or bowel), and thromboembolic disease. The risk of infant injury is low but not absent. The maternal morbidities may be in great part avoided, with greater awareness during the performance of the operation of the ultimate goal of returning uterine function to normal physiology. To a large extent, obstetricians hold the solution to the reduction of cesarean-related complications in their hands. The increasing performance of CS should never be regarded as the simplest means to solve most obstetrical difficulties. The relationship of a prior CS and subsequent conditions remotely connected necessitate further studies of various techniques and the adoption of specific surgical features to improve long term outcomes.
Cesarean morbidity has predominantly focused on short, rather than long-term maternal risks and outcomes. Women undergoing a cesarean birth are at increased risk of a variety of chronic and life-threatening conditions. These conditions increase with the increasing number of CDs. In the non-pregnant state, these include pain, adhesions, irregular bleeding and infertility. The pregnancy related risks include CSP and PAS, which represent the most deadly maternal complications in obstetrics. Increasing attention recently has addressed alterations in the infant microbiota induced by CS compared with vaginal birth, with long term consequences for obesity, and immune disorders such as asthma, allergy and atopic dermatitis.
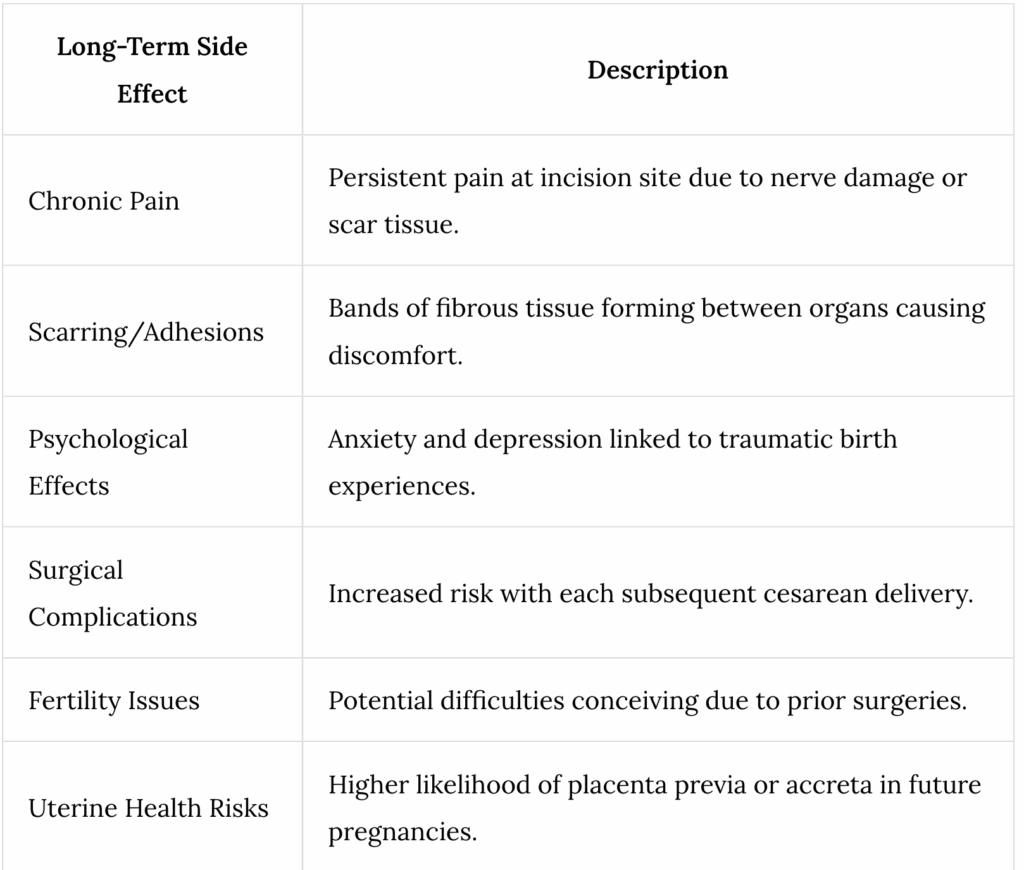
Nearest mention – Long-Term Side Effects Long-term complications from a C-section can affect different aspects of life.
Veteran (!!!) Muscle Recovery: Prolonged recovery may be necessary to regain full abdominal strength.
Adhesion Formation: Scar tissue can lead to future pregnancy complications or abdominal issues.
Impact on Future Pregnancies: Increased likelihood of requiring repeat C-sections and complications in subsequent pregnancies.

If you wish to keep looking – https://www.sciencenordic.com/denmark-videnskabdk-womens-health/c-sections-can-cause-complications-for-surgery-later-in-life/1448923
WHAT ABOUT THIRD WORLD? The magnitude of maternal complication of cesarean section was higher than most studies. Living in rural setting, having obstetric complications, previous cesarean scar, emergency surgeries, operation done in second stage of labor and prolonged duration of surgery are important predictors of maternal complication. Therefore, we recommend timely and adequate progress of labor evaluation, timely decision for cesarean delivery and vigilant care in post-operative period shall be conducted.
FINALLY – Abstract: Childbirth is a major event which can affect women’s quality of life, and giving birth by caesarean section may induce long-term health problems. Among those, during the first year, fatigue and back pain are more often reported than after a vaginal delivery. In contrast, postpartum depression concerns around 10% of the women whatever the mode of delivery. The incidence of chronic post surgical pain after caesarean section ranges from 4 to 9% in prospective studies which have excluded preexisting pain conditions, with 2% of women reporting severe pain. Scar pain predominates and very often presents with neuropathic features (50–60% of the cases at 6 months and still 26% of the cases at 12 months). Deep visceral pain is also mentioned and specifically chronic pelvic pain (incidence of 2.9% at 6 months and 1.3% at 12 months). Further, caesarean delivery seems associated with a reduced risk of chronic pelvic pain by comparison with vaginal delivery. Finally, previous caesarean section represents a significant risk factor for the development of chronic post surgical pain after hysterectomy performed later in life. While the degree of tissue trauma has only short-term impact, long-lasting problems, specifically chronic pain, are more related to individual predisposition. It is worth noting that, although they acknowledge needing help and advices, a majority of women do not consult health professionals. It is then mandatory that women’s health after childbirth becomes a priority as shared responsibility between the caregivers and the mothers.
MY CONCLUSION – no one is looking at the WHY – that is the nutrients and the engineering – that would be Vit D 3 to begin with , , ,
And where to find this info? Is not about WORST NEGLIGENT EXCLUSION – adenomyosis .AND THIS IS THE BEST WE CAN ACCESS? The excruciating pain is the issue – A and E – and on the floor, in ambulance and off your head on fentanyl – why not call it what it is – the body has been broached and the endometrial tissue in now WITHIN the walls of the womb – only can happen if there has been an actual breach into integrity – so that would be a C section – or