This is NOT PMT/PMS

It is often a life trashed
PMDD (premenstrual dysphoric disorder) is a life in two parts – before and after ovulation. Bipolar like. The Jekyl and Hyde situation. Night and day. Let us investigate:
WHY? What we make hormones with
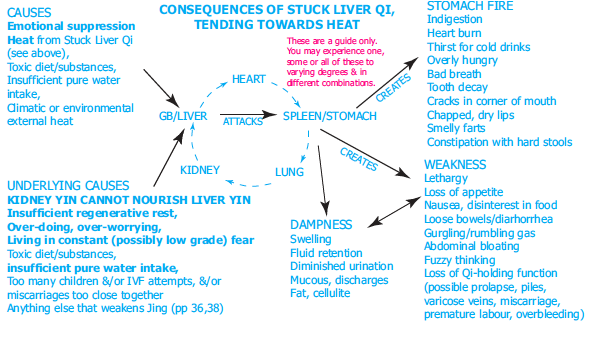
What gets us eventually – the STUCK Liver Qi grows, festers and over time – will erupt.
Monthly when cycling/having periods
In clinic, to understand the progression of this:
I went back to why them . .
And found all had had a sexual fright . . .
We as girls/women are supposed to smile and shut up. That stuffing things down will eventually end up as a ‘hormonal’ excuse as the biomedical people have drugs for this.
Retail opportunities BUT these do nothing to clear WHY this is happening . .
Stuck on drugs? Maybe see what else is possible.
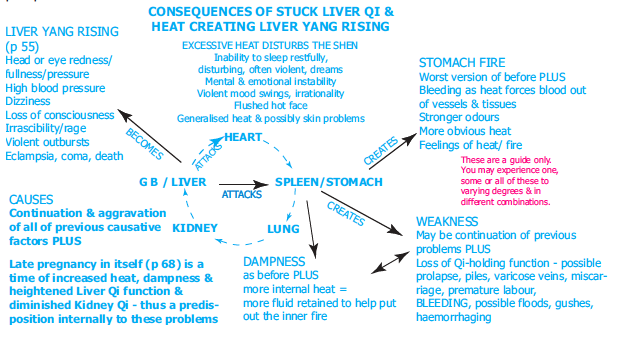
This is way past ‘stressed’ – it grows into INNER WIND – after picking up so much HEAT – see about this here.
BUT – what really needs to be is FIX the why . . .
To not listen to the ‘we don’t know’ brigade say ‘we don’t know’ AGAIN as we, with women DO ..
PISSED OFF – grows into fury and rage – and then ‘anxiety’ – will we kill in a moment of release?
Some of the ‘how’ . . . from my 2005 manual What Dads Can Do – which is essentially the text book I use for my students.
It is written for a pregnant audience – but periods grow into this – and when one is in a state of disorder, the rest will follow – likely not easily. We easily get into PND/PNP . . .and mad mamas may also be a part of this – what happens? Often past sexual ab-use becomes known in the birthing process – what a horror for the new born baby and mother – and family!!
It grows – and will be all that HOT HEADED/maniac sometimes – reactivity that is there a bit in PMS – this is combined in East Asian medicinal terms with DAMP and thus ‘madness’. Women with this – feel as though they are taken over – and may have no control. The worst thing is to numb it – as it WILL not go away by itself.. . ..
A multi modality approach is needed to GENTLY undo this
An unusual answer that may be a simple supplement – as well as the B complex – and as many all through the day as you can. Many of us have pyroluria (inability to absorb zinc and B 6) so this may also nee d to be investigated. . myo-inositol,
Inositol, or more precisely myo-inositol, is a carbocyclic sugar that is abundant in brain and other mammalian tissues, mediates cell signal transduction in response to a variety of hormones, neurotransmitters and growth factors and participates in osmoregulation. “Several studies have proposed a selective serotonin reuptake inhibitor-like role for myo-inositol, likely due to the fact that myo-inositol is the second messenger of serotonin”.
Allied to P.C.O.S. (As usual ‘we don’t know what causes it” .. .).
Even though ‘we don’t know what causes it -see fibromyalgia from where it all starts – back to the hormonal mud map and here
Instead there be drugs . .
Side effects of treatments
 All medicines have side effects. These are some of the side effects of treatment for PCOS.
All medicines have side effects. These are some of the side effects of treatment for PCOS.
1 – Ginet 84
GINET is used to treat women with acne, hair loss or increased growth of facial and body hair if these conditions are the result of over-production of male-typehormones called androgens. GINET contains two substances that act against the androgens, cyproterone acetate and ethinylestradiol. As well as being an anti androgen, cyproterone acetate acts like the female sex-hormone progestogen, and when combined with an estrogen(as in GINET, with ethinylestradiol),is an oral contraceptive for women being treated for androgen-dependent symptoms; however, GINET is not recommended in women solely for contraception. GINET can also be used to treat polycystic ovary syndrome, a hormone imbalance that can cause irregular or absent periods, acne ,excessive hair growth, infertility, recurrent miscarriage and obesity. Your doctor may have prescribed GINET for another purpose. Ask your doctor if you have any questions why GINET has been prescribed’.
- Nausea (feeling sick).
- Sore breasts.
- Occasional headaches.
- Increased risk of blood clots (deep vein thromboses) – especially if you’re overweight or a smoker.
- Signs include leg pain or swelling, chest pain, and shortness of breath.
2 – Spironolactone
- Nausea.
- Having to urinate (pee) more – this usually only lasts for a few days.
- Irregular periods.
3 – Cyproterone acetate
- Tiredness.
- Depression.
4 – Metformin
- Nausea (feeling sick).
- Abdominal (tummy) pain.
- Diarrhoea (the runs).
These side effects are less severe if you start on a low dose and build up gradually. People with severe heart, lung, liver or kidney problems shouldn’t take metformin. You shouldn’t take it on days when you’re ‘sick’. SO MUCH FOR THE ‘WE DON’T KNOW BRIGADE ‘ (medicos) and their thoughts ..
WHY NOT UNDO WHAT HAS HAPPENED TO THE ‘FEELINGS’ and let the body become aligned – intensive bundles of care now look like they are the only way – surely – after seeing the L.L.II. recipients of care . . Being there as the person traverses the mountains and valleys of their journey.
MAYBE ALLIED
Polycystic ovary syndrome (PCOS)

WHAT IS IT? A hormonal disorder causing enlarged ovaries with small cysts on the outer edges.
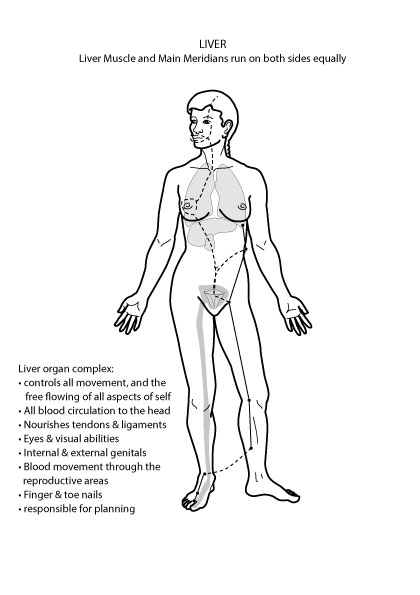
This is a medical version of Liver Fire (H’S opinion) PCOS is a condition that affects a woman’s hormone levels.
Women with PCOS produce higher-than-normal amounts of male hormones. (testosterone will be shown as libido possibly) This hormone imbalance may cause them to skip menstrual periods – H – often for years
Symptoms: Hair loss; Depression (mood); Acne
Risk Factors: Infertility; Diabetes; Obesity…
WHY? The cause of polycystic ovary syndrome isn’t well understood, but may involve a combination of genetic and environmental factors.
Symptoms include menstrual irregularity, excess hair growth, acne and obesity. (H – not always they can be thin and overly active /male shaped)
Medical treatments include birth control pills to regularise periods, medication called metformin to prevent diabetes, statins to control high cholesterol, hormones to increase fertility and procedures to remove excess hair.
NOTE – NONE OF THIS ADDRESSES WHY PCOS IS THERE – as the medicos do not know. BUT – will engage the woman in life long mischief – as usual
CYSTS? Iodine – see more in the Nourishing YOU and LIEF Essentials online courses. .

The nutritional is ONE aspect see more on Vit B 8 (inostol) here – if this is missing, it can be miraculous
Benefits of Myo-Inositol (Vit B8) for (PCOS)
Polycystic Ovary Syndrome
Myo-Inositol & PCOS
Polycystic ovary syndrome is the most common endocrine disorder and the cause of up to 30% of infertility in couples seeking treatment. It is commonly underdiagnosed and may affect up to as many as 15% of females during reproductive years. Research carried out at South Australia’s University of Adelaide and published in The Lancet has predicted that the global scale of this disorder is set to worsen.1
In this research review article, we take a closer look at a lesser-known natural compound called myo-inositol that has been found to have significant potential to improve many of the prevalent features of PCOS.
What is PCOS? FIRE in the Liver meridians
Where did this come from??? Not mentioned – LIFE
Here is the medical version of what is easily undone
IF we undo the why . . not medicate it.
ALL OF THIS IS TAKEN FROM AN UNUSUAL ALTERNATIVE – INOSITOL. .
‘The term ‘polycystic ovary syndrome’ (PCOS) describes a complex disorder with a range of symptoms. There is no single known cause and it is likely to be caused by a combination of genetic and environmental factors. It is characterised by chronic anovulation and excess ovarian activity, with the main feature being the presence of multiple underdeveloped tiny sacs (follicles) on the ovaries – often these underdeveloped follicles are unable to release an egg which means ovulation doesn’t take place.‘
‘In addition, a large proportion of women also have excessive androgen secretion or activity (hyperandrogenism) and abnormal insulin activity.2 Many body systems are affected in polycystic ovary syndrome resulting in several health complications which may include menstrual dysfunction, infertility, miscarriage, acne, oily skin, depression, obesity, hirsutism, hair loss, insulin resistance and increased risk of metabolic syndrome, cardiovascular disease, non-alcoholic fatty liver disease and chronic low grade inflammation.2,3
‘In 2003, The Rotterdam consensus defined the diagnostic criteria of PCOS as the presence of any two of the following three features: hyperandrogenism (clinical or biochemical), ovulatory dysfunction (often manifested by menstrual irregularities), and polycystic ovarian morphology (PCOM) by ultrasound. The Rotterdam criteria remains the most used diagnostic criteria for both individual diagnosis and research and yet is still generally accepted to have limitations.’In 2003, The Rotterdam consensus defined the diagnostic criteria of PCOS as the presence of any two of the following three features: hyperandrogenism (clinical or biochemical), ovulatory dysfunction (often manifested by menstrual irregularities), and polycystic ovarian morphology (PCOM) by ultrasound. The Rotterdam criteria remains the most used diagnostic criteria for both individual diagnosis and research and yet is still generally accepted to have limitations.
‘Needless to say, polycystic ovary syndrome is complex, commonly difficult to diagnose and is often missed completely.4,5
‘Nutrition & PCOS
The good news is that targeted dietary and lifestyle changes can be of significant help to women affected by this debilitating disorder. Whilst every case is unique, and requires an individualised and multi-faceted approach, effective treatment protocols commonly centre around the nutritional support of these four key areas:’Nutrition & PCOS
The good news is that targeted dietary and lifestyle changes can be of significant help to women affected by this debilitating disorder. Whilst every case is unique, and requires an individualised and multi-faceted approach, effective treatment protocols commonly centre around the nutritional support of these four key areas:
1. Weight management
2. Blood sugar balance and insulin function normalisation
3. Hormone balance
4. Ovarian health support
Patients often experience significant improvement in symptoms when these areas are addressed with targeted dietary and lifestyle strategies, and supplementation with specific nutrients and botanicals.
Myo-inositol is one supplement in particular which has received widespread attention for the potential role it has to play in supporting women with PCOS. And much research to date indicates that this novel supplement has the potential to provide support for many of these key areas.
What is Myo-inositol?
Myo-inositol is one of nine different types of inositol. It is a naturally occurring substance produced in the human body from glucose, although it is not a sugar. Better described as a ‘vitamin-like’ substance, myo-inositol is often considered to be a member of the B complex group of vitamins. However, because it is produced by the body in amounts considered sufficient to support health, it is not officially termed an essential nutrient. In addition to the body’s own production from glucose, myo-inositol is also found naturally in many foods such as organ meats, fruit, grains, nuts and beans.
Myo-inositol – Key role in insulin signalling
Myo-inositol is involved in the metabolism, transport and breakdown of glucose and its conversion to glycogen. It is a key factor involved in insulin signalling, and is an immediate precursor to another type of inositol, D-chiro-inositol, which interacts with select sugars in the body to form inositol phosphoglycans – these play an important role in mediating the actions of insulin.6-12 Low levels of myo-inositol, D-chiro-inositol and inositol phosphoglycans have been observed in individuals with impaired insulin sensitivity and PCOS.6-12
Myo-inositol & PCOS
A number of recent studies have found myo-inositol to be an effective support in PCOS, in part due to its ability to improve insulin sensitivity, restore hormonal balance, improve menstrual regularity, reduce hyperandrogenism and influence ovarian function. Research has also demonstrated fertility-improving effects of myo-inositol among women with PCOS; and since the syndrome is the leading cause of female infertility, these results are particularly encouraging.13-22
So, what’s the evidence?
• In a 2009 double blind clinical trial, 42 women with PCOS received myo-inositol (4 grams daily plus 400mcg folic acid) or placebo (folic acid alone). Results showed that myo-inositol increased insulin sensitivity, improved glucose tolerance and decreased glucose-stimulated insulin release. In addition, the researchers noted a positive effect on ovulation – 16 out of 23 women in the myo-inositol group ovulated, compared to 4 out of 19 women in the placebo group. In these women, there was also a 66% reduction of serum total testosterone and a 73% reduction of serum free testosterone concentrations. Cardiovascular markers, systolic and diastolic blood pressures, plasma triglycerides and total cholesterol concentrations also decreased in the myo-inositol group.13
• Another study in 20 overweight women with PCOS found that 12 weeks of supplementation with myo-inositol improved insulin sensitivity and reproductive hormone balance and completely restored the menstrual cycle in all amenorrheic and oligomenorrheic subjects.14
• Research carried out in 2011 showed a combination of the contraceptive pill and myo-inositol (4 grams daily for 12 months) to be more effective in controlling the endocrine, metabolic and clinical profile in patients with PCOS than the contraceptive pill alone; the same study also found myo-inositol reduced insulin levels and insulin resistance.15
• In a prospective clinical study carried out in Rome in 2008, researchers investigated the effects of myo-inositol on two of the most common features of PCOS, hirsutism and hyperandrogenism. In the study, 46 women were evaluated at baseline and then again, following treatment with myo-inositol for 6 months. Results showed that treatment with myo-inositol significantly reduced hirsutism, hyperandrogenism and insulin resistance.16
Learn More
• SUPPLEMENTS: Inositol & Myo-Inositol Range
• FERTILITY: How Myo-Inositol Supports Fertility
• MAGNESIUM FOCUS: Magnesium, PMS & Menopause
• In a double blind trial published in 2011 in the European Review for Medical and Pharmacological Sciences, researchers compared the effects of supplementation with 2g myo-inositol and 200 mcg folic acid compared to 200 mcg folic acid taken twice daily for 3 months in women with PCOS undergoing IVF and ovulation induction. At the end of the treatment, in the group taking myo-inositol, both the number and quality of oocytes (immature egg cells) was greatly improved. The authors concluded, “these data suggest that myo-inositol may be useful in the treatment of PCOS patients undergoing ovulation induction, both for its insulin sensitizing activity, and its role in oocyte maturation.”17 Additional research has found myo-inositol to be useful for improving oocyte quality, ovulation and pregnancy outcomes.18-22
• In a 2018 randomised controlled trial published in the Journal of Psychosomatic Obstetrics and Gynaecology researchers compared the effects of 12 weeks of intervention with either myo-inositol or metformin on mental health parameters and biomarkers of oxidative stress in 60 subjects with PCOS. Results showed that after the 12-week intervention, changes in general health, depression, anxiety & stress, and plasma total antioxidant capacity (TAC) concentrations in the myo-inositol group were significantly different from the changes in these indicators in the metformin group. The researchers concluded that their data supported that myo-inositol supplementation for 12 weeks among patients with PCOS has favourable effects on parameters of mental health and plasma TAC levels.23
• In a 2017 randomised controlled trial published in Gynecological Endocrinology, researchers compared the effects of metformin and myo-inositol on the clinical and metabolic features in PCOS. Fifty women with PCOS and either insulin resistance or hyperinsulinaemia were randomised to receive treatment with either metformin (1500 mg/day) or myo-inositol (4g / day). Results in both groups were similar: insulin sensitivity and BMI significantly improved in both groups, and the menstrual cycle was normalised in about 50% of the women. The researchers concluded that both metformin and myo-inositol have been demonstrated to be useful in women with PCOS for lowering BMI, improving insulin sensitivity, and improving menstrual cycle, without significant differences between the two treatments.24
• In a 2017 review on using inositols in PCOS, and published in Gynecological Endocrinology, the authors found combined treatment with myo-inositol and d-chiro inositol to be effective in restoring ovary function and metabolic balance in PCOS.25
• A 2017 randomised controlled trial was carried out to compare the effects of metformin and myo-inositol on clinical, metabolic and genetic parameters in women with PCOS. The researchers concluded that, “overall, taking myo-inositol, compared with metformin, for 12 weeks in patients with PCOS with hyperinsulinism and normoinsulinism had beneficial effects on total testosterone, mFG scores, serum hs-CRP levels and gene expression of IL-1, but did not affect other hormonal profiles, NO levels or gene expression of IL-8 and TNF-α.”26
• A 2017 randomised controlled crossover study was carried out to investigate which is more effective between metformin and myo inositol on hormonal, clinical and metabolic parameters in obese patients with PCOS. In the study, 34 PCOS obese women were randomised to receive metformin (850mg twice daily) or myo-inositol (1000mg twice daily) for 6 months. After a 3-month washout period, the same subjects received the other compound for the following 6 months. Results showed that both treatments improved the glyco-insulinaemic features of obese PCOS patients, but only metformin seems to exert a beneficial effect on the endocrine and clinical features of the syndrome.27
Myo-Inositol – From Research to Clinical Application
As you will no doubt be gathering by now, there is significant potential for the use of myo-inositol. For women suffering with the many debilitating faces of PCOS; from insulin resistance to excess androgens, anovulation and more, myo-inositol has the potential to offer significant and wide-ranging benefits. And whilst myo-inositol has demonstrated significant benefits in women with PCOS, its use is not limited here.
Myo-inositol may be of benefit for a range of applications related to female health, and additional research in the area has found this to be the case. Clinical studies have shown benefits of using myo-inositol in patients with premenstrual dysphoric disorder (a severe form of PMS) and in postmenopausal women with metabolic syndrome.28-30 Research shows that myo-inositol also has an integral role in the activation of serotonin receptors (the ‘feel-good’ neurotransmitter), thus supporting its use for mood balance in the premenstrual phase of the menstrual cycle and also potential uses in depression and panic disorder.31
The clinical applications of myo-inositol are already wide ranging and it’s likely, as research in the area gathers momentum, more may be added. For women with PCOS though, research shows that myo-inositol is a useful consideration as part of their treatment protocol.
Myo-Inositol – How much to take?
Current research suggests that for women with PCOS, 2000mg myo-inositol combined with folic acid, taken 1-2 times daily for 3 months is an effective protocol to begin with before reviewing the programme.13-22 32 Clinical doses of myo-inositol may be best achieved in supplemental powdered form. The benefits demonstrated by research so far have involved myo-inositol in supplemental form rather than from food sources; it is also unlikely that food sources can supply high enough levels to achieve a therapeutic effect.
Myo-Inositol – Is it safe?
Myo-inositol appears to be safe and well tolerated by most. There have been some mild reported side effects in the scientific literature, which include mild gastrointestinal side effects such as nausea, flatulence and diarrhoea, and dizziness, tiredness and headache32-35 but these appear to occur at doses higher than are generally recommended. Patients with bi-polar disorder are also advised to avoid supplementation with myo-inositol before further research can determine its safety.32-35 As with all supplementation, patients with existing medical conditions or taking prescribed medication should always consult a healthcare practitioner before starting to take myo-inositol.
Myo-inositol – A promising emerging support for PCOS…
Currently, the evidence to support using myo-inositol in PCOS is rapidly emerging and promising particularly with regard to hormonal, ovulatory and metabolic benefits. As with many aspects of nutrition-based interventions however, the research is still considered to be limited by small study group sizes. According to the International PCOS Network, inositol (in any form) should be considered an experimental therapy in PCOS, “as this agent is freely available as a nutritional supplement, at low to moderate cost and appears to have a limited side effect profile, it may warrant consideration for use despite limited and low quality evidence. As with other supplements or complementary therapies, women taking this agent are encouraged to advise their health care team.”36
References:
1. Norman RJ, Dewailly D et al. Polycystic ovary syndrome. The Lancet, Volume 370, Issue 9588, Pages 685-697, 25 August 2007 doi. 10. 1016/S0140-6736(07) 61345-2
2. Hirschberg AL. Polycystic ovary syndrome, obesity and reproductive implications. Womens Health (Lond Engl). 2009 Sep; 5(5):529-40
3. Rocha AL, Oliviera FR et al. Recent advances in the understanding and management of polycystic ovary syndrome. F1000 Research. 2019 Apr 26; 8: F1000 Faculty-Rev-565
4. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group: Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004; 81(1):19–25.
5. Wang R, Mol BW: The Rotterdam criteria for polycystic ovary syndrome: evidence-based criteria? Hum Reprod. 2017;32(2):261–4.
6. Susuki S et al. Urinary chiro-inositol excretion is an index marker of insulin sensitivity in Japanese type II diabetes. Diabetes Care. 1994 Dec;17(12):1465-8.
7. Jung TS et al. Determination of urinary Myo-/chiro-inositol ratios from Korean diabetes patients. Yonsei Med J. 2005 Aug 31;46(4):532-8.
8. Cheang KI, Baillargeon JP, Essah PA, et al. Insulin-stimulated release of D-chiro-inositol-containing inositol phosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome. Metabolism. 2008 Oct; 57(10): 1390-7.
9. Baillargeon JP, Iuorno MJ et al. Uncoupling between insulin and release of a D-chiro-inositol-containing inositol phosphoglycan mediator of insulin action in obese women with polycystic ovary syndrome. Metab Syndr Relat Disord. 2010 Apr;8(2):127-36.
10. Croze ML, Soulage CO. Potential role and therapeutic interests of myo-inositol in metabolic diseases. Biochimie 2013 95 1811–1827. 10.1016/j.biochi.2013.05.011
11. Genazzani AD, Prati A, Santagni S, et al. Differential insulin response to myo-inositol administration in obese polycystic ovary syndrome patients. Gynecol. Endocrinol. 2012. 28 969–973.
12. Unfer V, Carlomagno G, et al. Effects of myo-inositol in women with PCOS: a systematic review of randomized controlled trials. Gynecol. Endocrinol. 2012. 28 509–515.
13. Costantino D, Minozzi G et al. Metabolic and hormonal effects of myo-inositol in women with polycystic ovary syndrome: a double-blind trial. Eur Rev Med Pharmacol Sci. 2009 Mar-Apr;13(2):105-10.
14. Genazzani AD, Lanzoni C et al. Myo-inositol administration positively affects hyperinsulinemia and hormonal parameters in overweight patients with polycystic ovary syndrome. Gynecol Endocrinol. 2008 Mar;24(3):139-44.
15. Minozzi M, Costantino D et al. The effect of a combination therapy with myo-inositol and a combined oral contraceptive pill versus a combined oral contraceptive pill alone on metabolic, endocrine, and clinical parameters in polycystic ovary syndrome. Gynecol Endocrinol. 2011 Nov;27(11):920-4.
16. Minozzi M, D’Andrea G et al. Treatment of hirsutism with myo-inositol: a prospective clinical study. Reprod Biomed Online. 2008 Oct;17(4):579-82.
17. Ciotta L, Stracquadanio M, et al. Effects of myo-inositol supplementation on oocyte’s quality in PCOS patients: a double blind trial. Eur Rev Med Pharmacol Sci. 2011 May; 15(5): 509-14.
18. Rizzo P, Raffone E, Benedetto V. Effect of the treatment with myo-inositol plus folic acid plus melatonin in comparison with a treatment with myo-inositol plus folic acid on oocyte quality and pregnancy outcome in IVF cycles. A prospective, clinical trial. Eur Rev Med Pharmacol Sci. 2010 Jun;14(6):555-61.
19. Papaleo E, Unfer V, et al. Myo-inositol may improve oocyte quality in intracytoplasmic sperm injection cycles. A prospective, controlled, randomized trial. Fertil Steril. 2009 May;91(5):1750-4.
20. Papaleo E, Unfer V et al. Myo-inositol in patients with polycystic ovary syndrome: a novel method for ovulation induction. Gynecol Endocrinol. 2007 Dec;23(12):700-3. Epub 2007 Oct 10.
21. Gerli S, Mignosa M, et al. Effects of inositol on ovarian function and metabolic factors in women with PCOS: a randomized double blind placebo-controlled trial. Eur Rev Med Pharmacol Sci. 2003 Nov-Dec; 7(6):151-9.
22. Papaleo E, Unfer V et al. Myo-inositol in patients with polycystic ovary syndrome: a novel method for ovulation induction. Gynecol Endocrinol. 2007 Dec; 23(12):700-3.
23. Jamilian H, Jamilian M et al. Comparison of myo-inositol and metformin on mental health parameters and biomarkers of oxidative stress in women with polycystic ovary syndrome: a randomised, double-blind, placebo-controlled trial. J Psychosom Obstet Gynaecol. 2018 Dec; 39(4): 307-314
24. Fruzzetti F, Perini D, et al. Comparison of two insulin sensitizers, metformin and myo-inositol, in women with polycystic ovary syndrome (PCOS). Gynecol Endocrinol. 2017 Jan; 33 (1): 39-42
25. Monastra G, Unfer V, Harrath AH, et al. Combining treatment with myo-inositol and D-chiro-inositol (40:1) is effective in restoring ovary function and metabolic balance in PCOS patients. Gynecol Endocrinol. 2017;33(1):1–9.
26. Jamilian M, Farhat P, Foroozanfard F, et al. Comparison of myo-inositol and metformin on clinical, metabolic and genetic parameters in polycystic ovary syndrome: A randomized controlled clinical trial. Clin Endocrinol (Oxf). 2017;87(2):194–200.
27. Tagliaferri V, Romualdi D, Immediata V, et al. Metformin vs myo-inositol: which is better in obese polycystic ovary syndrome patients? A randomized controlled crossover study. Clin Endocrinol (Oxf). 2017;86(5):725–30. 10.1111/cen.13304
28. Gianfranco C, Vittorio U, Silvia B, Francesco D. Myo-inositol in the treatment of premenstrual dysphoric disorder. Hum Psychopharmacol. 2011 Oct; 26(7):526-30.
29. Cunningham J, Yonkers KA, et al. Update on research and treatment of premenstrual dysphoric disorder. Harv Rev Psychiatry. 2009; 17(2):120-37.
30. Giordano D, Corrado F, et al. Effects of myo-inositol supplementation in postmenopausal women with metabolic syndrome: a perspective, randomized, placebo-controlled study. Menopause. 2011 Jan;18(1):102-4
31. Benjamin J, Agam G, et al. Inositol treatment in psychiatry. Psychopharmacol Bull. 1995;31(1):167-75.
32. Carlomagno & Unfer (2011), Inositol safety: clinical evidences. Eur Rev Med Pharmacol Sci, 15: 931-936
33. Nierenberg AA, Ostacher MJ et al. Treatment-resistant bipolar depression: a STEP-BD equipoise randomized effectiveness trial of antidepressant augmentation with lamotrigine, inositol, or risperidone. Am J Psychiatry. 2006; 163: 210–216.
34. www.webmd.com
35. Lovieno, N, Dalton, ED et al. Second-tier natural antidepressants: Review and critique. Journal of Affective Disorders. 130 (2011): 343-357.
36. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod. 2018;33(9):1602–18.